

What is DPC data? Some Explanations about techniques for best usage, analysis methods, and differences with receipt data
Do you know “DPC data”? Even if you know the word somehow, there are few people who understand the meaning and where it applies.
In this article, we would like to provide:
- An explanation of “DPC” and terms related to DPC
- A description of DPC data content & meaning
- DPC data analysis methods and utilization techniques
Our explanation is in plain language, avoiding technical jargon and complex representations. Thanks to our illustrations and diagrams, we hope that you will get the full meaning of it.
What is DPC?
First of all, we should explain what the acronym stands for and what is the meaning of the word “DPC”. DPC is an abbreviation for “Diagnosis Procedure Combination”. It refers to the combination of diagnosis and procedure inside the hospitals.
For example, we classify patients according to their “diagnosis” and “treatment content,” with the image of creating a combination classification where the vertical axis is the diagnosis and the horizontal axis is the treatment content.
This DPC is a relatively new concept and is based on the “DPC system”, what refers to DPC/PDPS (Diagnosis Procedure Combination/Per-Diem Payment System) and was introduced in 2003 in Japan. This refers to the system for a comprehensive evaluation of hospital care per patients in the acute phase (conditions requiring immediate treatment) at large hospitals that meet certain criteria.
“Comprehensive” means that the system adopts a flat-rate remuneration principle instead of the performance-based remuneration system that was used before the DPC system was introduced.
Essentially, medical care should provide patients with efficient, cost-effective, and high-quality medical care, but there are times when this logic can hardly apply because the human factor is involved.
In the performance-based remuneration system (performance-based payment), hospitals were incentivized to operate more tests and treatments, as it would provide resources to the hospital, but at the detriment of the patient, making impossible a “patient-first” medical care policy.
Therefore, by adopting the DPC system and making it a “fixed amount” remuneration system, medical professionals put patients first and emphasize cost performance. Hospitals can realize the medical treatment aiming at:
- Early discharge of patients
- Use of drugs that are as cost-effective as possible
- Minimum necessary inspection
What is DPC data
The data generated as a result of DPC calculation among the hospitals subject to DPC mentioned above is called “DPC data”.
This definition of DPC data excludes data from hospitals and clinics that do not handle DPC in the first place.
Each patient’s DPC data is classified and summarized by a number called a “DPC code”.
The DPC code is a 14-digit number used to determine the “hospitalization fee”.
One patient is given one code and there are no duplicate.
For example, if you are hospitalized with two illnesses, such as “I fell and broke my arm while hospitalized with pneumonia,” the code with the higher treatment cost will be selected.
What is the DPC Code?
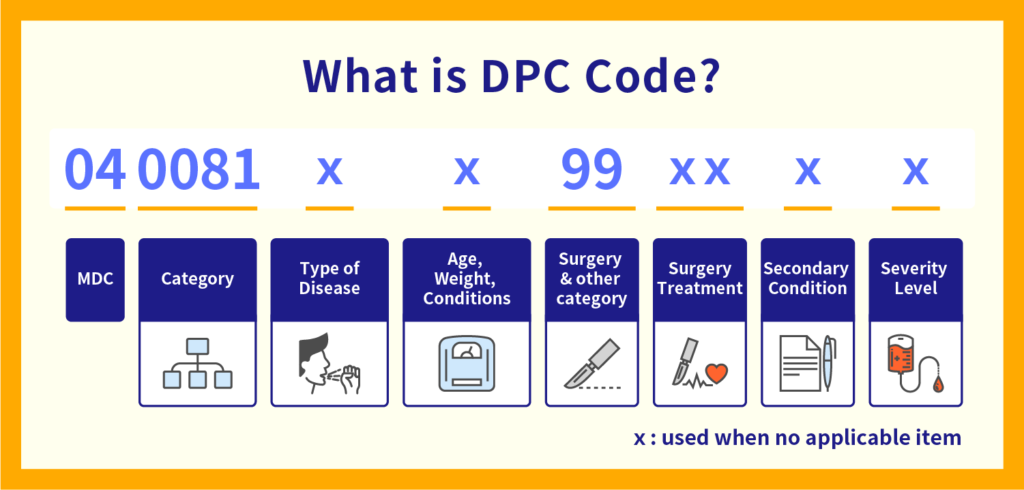
The DPC code is designed to identify several parameters supporting the identification of the patient and the description of the treatment handling:
The first 6 digits indicate “the disease that invested the most medical resources during hospitalization,” and is called the “basic DPC”.
A code is determined for each disease. For example, if you are hospitalized for aspiration pneumonia, it will be encoded as “040081”. The first two digits of these six digits are called MDC (major disease category), which simply indicates “what family of disease it belongs to”. In the case of aspiration pneumonia, it becomes a respiratory disease and is written as 04.
The 7th digit represents the classification of pathology, etc., but since 2006, this classification has not been revised.
The 8th digit may be entered when age, birth weight, and JCS (classification of disturbance of consciousness) affect the content of treatment.
The 9th and 10th digits are called “surgical subclassifications” and are assigned according to the surgery for each disease based on the basic DPC. If surgery is not required, such as for aspiration pneumonia, it will be encoded as “99”.
The 11th / 12th digits may be assigned when other treatments (radiation therapy, chemotherapy, etc.) are performed besides surgery.
The 13th / 14th digits are assigned according to the severity of other illnesses that occurred during hospitalization.
What is the content of DPC Data?
In this part, we would like to describe the concrete meaning of the data. DPC Data could be categorized as shown in the table below:
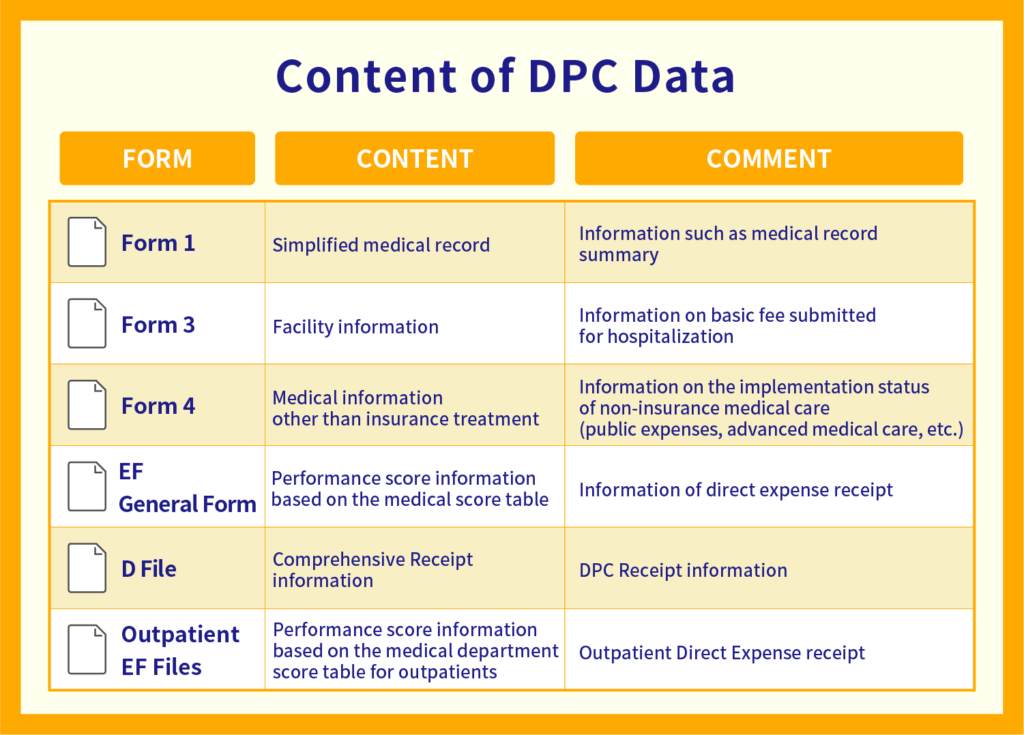
DPC data are used to proceed with the reporting of the treatment procedure associated with a clearly defined and proven diagnosis so the structure of data corresponds to the different administrative forms that DPC hospitals are required to submit.
The “Form 1 file” is the patient’s individual information, such as the “discharge summary” where the doctor summarizes the patient’s hospitalization information at the time of discharge, such as the state of consciousness at the time of admission, date of birth, discharge destination, name of disease, etc.
The “Form 3 file” describes “Information such as facility usage expenses other than medical treatment” for example the basic hospitalization fee and the fee for hospitalization itself.
The “Form 4 file” contains information on “payments other than remuneration for insurance medical treatment.”
The “EF file” contains information about drugs, such as the type and quantities of drugs used during hospitalization, or the number of days administered.
The “D file” summarizes the points (fees) for medical care during hospitalization, including examinations, medicines, and injections.
Main Features of the DPC database
DPC data is compiled into a “DPC database”, and its greatest feature is its “abundant patient data”.
As mentioned earlier, the strength of DPC data is that it can check various data such as the patient’s condition from the time of admission to the time of discharge, medical treatment, drugs used, points, etc.
“Data is limited to DPC hospitals” and “Basically limited to hospitalized data” are among the leading arguments pointing at a disadvantage, but conversely, it is difficult to study severe diseases that often require hospitalization at large hospitals. It can be said that it is very suitable data for specific research needs.
About DPC public data
There is a lot of information that can be learned from the DPC’s data publicly available. However medical practices such as:
- Surgery or anesthesia
- Radiation therapy
- Rehabilitation
- Complicated inspection behavior
That qualify as “Medical practices that may change the results depending on the skill of the provider (or the medical staff)” and “Medical practices that cause variations in the results of treatment” are based on a separate rate system and are not included in the DPC data. Therefore, not all medical practices are included in the DPC public data.
Nonetheless, by looking at the DPC data, it is possible to confirm to a certain extent how much hospitals provide “medical care” to “what kind of patients” and “how much income they receive.”
The difference between Receipt Data and DPC Data
We would like now to explain the difference between receipt data and DPC data.
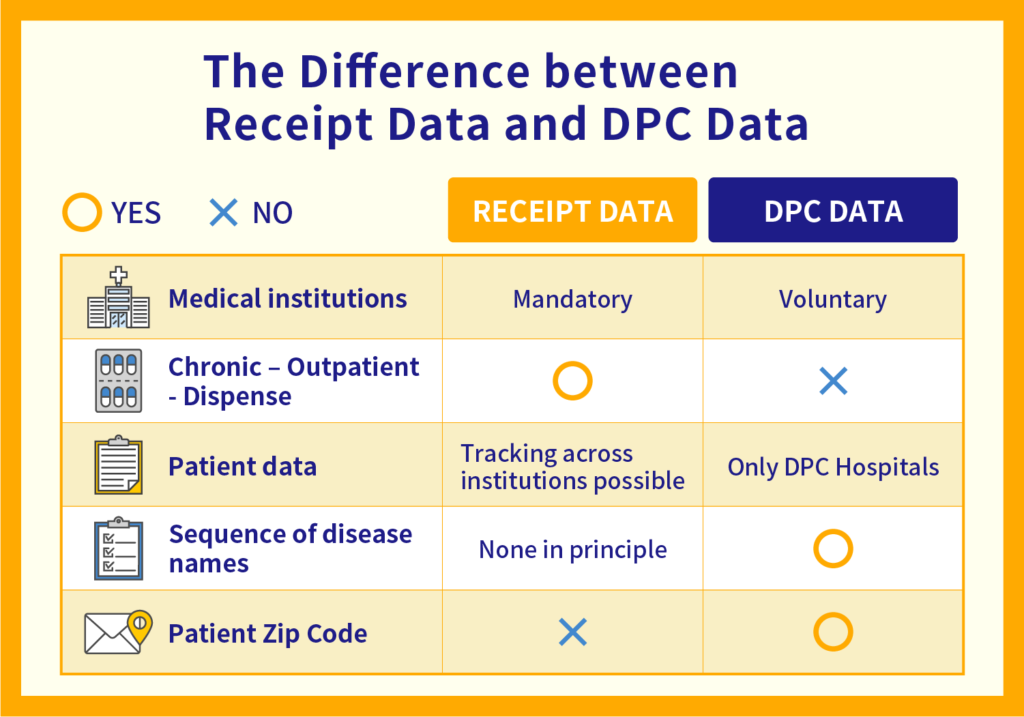
Receipt data is detailed data of “medical fees” such as what kind of illness a patient consulted for and what kind of treatment was received at a hospital, clinic, dispensing pharmacy, etc. There are some differences between DPC data and receipt data, but the major difference is their “coverage”.
DPC data is data only for hospitals that have made a bid to become DPC hospitals and have received approval, while receipt data is data for all insurance medical institutions inside and outside hospitalization, including chronic phases, local clinics, and dispensing pharmacies.
However, while the receipt data does not include the name of the disease or the postal code of the patient, the DPC data includes such items, so the advantage is that there is more detailed information.
What is the coefficient by medical institution?
Income from the DPC system varies from hospital to hospital, and it is related to the “medical institution coefficient”.
In other words, even if you do the same test B for the same disease A, the price will be different depending on the hospital. This “coefficient by medical institution” can be roughly divided into three categories:
1. Basic coefficient
The first is the “base factor”. This is very simple and it changes according to the rank of the hospital itself, and institutions are ranked following the order; University hospital > DPC designated hospital > DPC non-designated hospital.
2. Functional evaluation coefficient I
Next is “Function Evaluation Coefficient I”.
This is a coefficient that changes depending on the “work system”, for example how many nurses are assigned will affect the coefficient:
- Is there a lot of night shifts and is it getting longer?
- Are there sufficient personnel to assist the work of the doctor?
- Are medical safety measures and infection control measures in place?
It is used to evaluate if a medical institution has a system in place to provide medical care safely by securing sufficient personnel and taking measures to anticipate problems.
3. Functional evaluation coefficient II
The last one is “Function Evaluation Coefficient II”. This is a coefficient that changes depending on “how well the hospital is able to provide high-quality medical care.”
- How few mistakes are made when submitting a claim
- Is there a strong focus on efficiency and early discharge of patients?
- Are highly specialized and difficult surgery performed at the hospital?
- What is the effort allocation between emergency medical care and community medicine?
Hospital revenues are influenced by these three factors.
DPC data analysis methods and utilization techniques
Finally, we would like to explain how to analyze and utilize DPC data.
First, from the hospital’s point of view, comparison of DPC data from year to year can be used to improve management and lead to improvements in the quality of medical care itself. Thanks to the DPC database, even for the purpose of increasing profits, aiming for high-quality medical care without increasing the number of unnecessary tests should contribute to increased profits.
And for those who create the DPC system, the database provides a bird’s-eye view of which hospitals are providing what kind of quality medical care and how much income they are earning. This is very helpful data for healthcare management.
Although the target is limited, it is a database with more content than medical insurance claims data, so it is possible to imagine improving effective treatment and achieve better medical care by leveraging the tools that our company Medical Data Vision provides. Such tools analyzing treatment procedure vs. outcome and demographic surveys are widely used by healthcare companies, and research academy.
MDV collects DPC data from more than 400 facilities out of the nationwide DPC target hospitals (approximately 1,750); it represents a coverage rate of approximately 25%. Among the DPC data introduced at this time, the height and weight of the patient, the degree of progression of the cancer, the heart function, the liver function, etc. are as many parameters that can be used to check the severity; MDV tools and survey analysis are being used in various contexts, for example, by checking the EF data (medicine-related information) part of the DPC data, it is possible to grasp the types and volume of drugs used at the DPC hospital. Therefore, if you are a pharmaceutical company, you can effectively use it for market research, identifying what kinds of drugs are used for what kind of diseases and how much.
In addition, for academic research institutes, utilizing large-scale statistical information of critically ill patients with specific diseases hospitalized at DPC hospitals can greatly assist in clinical research. If you need to report to the government, you can create high-quality statistical data by referring to the patient information section of the DPC.
As you can see, there are many cases where MDV data has been used, so if you are considering the use of medical big data in your business, please do not hesitate to contact us.
For More Information, Please Contact Us Here
About Japanese Healthcare System

What you need to know about the healthcare system in Japan before using the data.
SERVICE

In addition to various web tools that allow you to easily conduct surveys via a browser using our medical database, we offer data provision services categorized into four types to meet your needs and challenges: "Analysis reports" "Datasets," "All Therapeutic Areas Data Provision Service," and "Specific Therapeutic Areas Data Provision Service.
![]()
© Medical Data Vision Co., Ltd. All Rights Reserved.