

How Real-World Data (RWD) is Shaping Clinical Trials in Japan
Japan is the world’s third-largest pharmaceutical market, valued at approximately USD 86 billion in 2025, a market too significant for global development teams to approach with assumptions carried over from the US or Europe. Trial teams here work within an aging population, complex treatment sequencing, and high standards of care that can make recruitment and endpoint selection harder than expected when protocols are imported with minimal local adjustment.
This is where real-world data (RWD) has become strategically important. Healthcare digitization has expanded access to claims datasets, electronic medical records (EMRs), and disease registries, including large-scale hospital databases covering over 60 million patients across 936 DPC hospitals. For sponsors planning a RWD clinical trial in Japan, this creates an opportunity to pressure-test trial assumptions early, using data that reflects routine practice rather than best-case scenarios.
Using RWD to strengthen trial design and feasibility in Japan

RWD is most valuable in the weeks and months before a protocol is finalized. Used early, it moves a team from expected feasibility toward planning grounded in real data.
Rather than relying on generalized benchmarks, sponsors can ground their decisions in data that reflects how patients are actually diagnosed, treated, and monitored within the Japanese healthcare system.
Evaluating patient availability and treatment pathways
A key starting point is understanding whether the target population is realistically accessible under proposed criteria.
Treatment patterns in Japan can differ from Western markets due to local guidelines, reimbursement structures, and prescribing behaviour. By analysing real-world data in Japan, sponsors can estimate how many patients are likely to meet proposed inclusion and exclusion criteria once real prescribing patterns and testing frequency are taken into account.
This is particularly important when eligibility depends on factors such as prior lines of therapy, biomarker testing rates, or the timing of treatment switches, areas where Japan may not mirror the US or EU. Without this validation step, studies risk being underpowered or delayed due to overly optimistic assumptions.
Understanding local practice patterns to refine criteria
Beyond patient counts, RWD helps clarify how care is actually delivered in practice. Recruitment delays often come down to eligibility criteria that look reasonable on paper but do not match the real patient population seen in practice, and RWD can highlight where criteria are unintentionally restrictive.
In some cases, small adjustments, such as aligning lab windows with routine monitoring schedules or refining prior therapy requirements, can materially improve feasibility without weakening the study question. These refinements are often subtle but can have a meaningful impact on recruitment timelines and site burden.
Anticipating recruitment bottlenecks and site capacity
RWD can also be used to move from high-level feasibility to operational planning. By identifying site-level patient volume, referral patterns, and regional variation in care delivery, teams can build a site shortlist based on data rather than assumptions, and anticipate operational bottlenecks before timelines are committed. In practice, it avoids the costly, time-consuming adjustments that tend to surface mid-study.
PMDA’s perspective on RWD in clinical development
As RWD becomes more integrated into global clinical development, understanding local regulatory expectations is critical. Japan’s Pharmaceuticals and Medical Devices Agency (PMDA) has signalled that RWD can be valuable as supportive evidence, particularly when conventional approaches are difficult to execute. In April 2021, PMDA established a dedicated RWD Working Group comprising experts from new drug review, safety, medical informatics, and epidemiology to address regulatory issues related to RWD utilization. This is especially relevant in oncology, rare diseases, and settings where patient populations are small or heterogeneous.
While randomized trials remain central to regulatory decision-making, PMDA has recognised that RWD can provide useful context on natural history, treatment patterns, and real-world outcomes in Japan. In practice, that makes RWD a complement to conventional trials rather than a substitute for them.
What PMDA expects: reliability and analytical transparency
A consistent theme in PMDA expectations is methodological discipline. Sponsors should be prepared to explain:
- Where the data comes from (and what it was originally collected for)
- How patients were selected and filtered
- Which variables are captured directly versus derived analytically
- How confounding, bias, and missingness were addressed
- Whether key fields are consistently recorded across hospitals or systems
Providing this level of clarity helps regulators assess whether conclusions drawn from RWD are robust and reproducible. These principles align with global RWE best practices, including those outlined by ISPOR and PMDA’s own guidance on ensuring the reliability of post-marketing database studies and registry data (see the PMDA RWD page).
RWD as part of regulatory consultations
Timing also plays an important role in how RWD is perceived. RWD is often most useful when introduced early, during feasibility discussions or protocol development, rather than added late as an afterthought. In PMDA consultations, well-framed RWD analyses can support design decisions (for example, choice of endpoints, inclusion criteria, or expected event rates) and provide context for how the study will perform in Japanese clinical practice. Early engagement allows for alignment on expectations and reduces the likelihood of rework later in development.
Japan’s most relevant RWD sources for clinical trial planning
With a growing number of data sources available, selecting the right dataset is a strategic decision. Japan offers several RWD sources that can support feasibility, protocol optimisation, and evidence planning; the right choice depends on the decision you are trying to make (population size, endpoint availability, site selection, or treatment sequencing). Understanding the strengths and limitations of each source is essential to avoid misapplication.
NDB claims data for population-level insight
At the population level, claims databases provide a broad view of healthcare utilisation. The National Database of Health Insurance Claims and Specific Health Checkups (NDB), maintained by Japan’s Ministry of Health, Labour and Welfare (MHLW), covers virtually the entire insured population and provides insights across a wide range of conditions and treatments.
NDB is useful for understanding prevalence, utilisation patterns, and broad treatment landscapes. However, access is tightly controlled, and clinical detail is limited compared with EMR-based sources, so it is often best used in combination with more granular datasets.
Hospital EMRs for clinical granularity
For more detailed clinical insights, hospital EMR datasets can offer richer clinical detail such as laboratory values, imaging results, and physician-recorded outcomes. These sources are often well-suited to feasibility assessments and protocol refinement, but they can vary by hospital system, coding practices, and completeness. Analytical standardisation is usually needed before results are comparable across sites; it adds work up front but makes the data far easier to interpret.
Disease registries (oncology and rare diseases)
In certain therapeutic areas, registries provide structured longitudinal data. Japan has disease registries that may support longitudinal analyses, particularly in oncology and rare diseases. Depending on the registry and governance model, these sources can be relevant for natural history work, post-marketing research, and external comparator development. Their value often lies in consistency over time rather than breadth of coverage.
Digital health and remote monitoring datasets
Emerging data sources are also beginning to complement traditional datasets. As remote monitoring tools and digital health platforms expand, these datasets may increasingly complement traditional RWD sources. While still emerging in many settings, they can help teams understand patient experience outside routine clinic visits and may support future hybrid trial designs.
Innovative trial applications enabled by RWD in Japan
Beyond feasibility, RWD is enabling more flexible and adaptive approaches to trial design. As confidence in real-world evidence grows, sponsors are exploring ways to incorporate RWD into both the structure and execution of studies.
External control arms for small or rare populations

A prominent example is the external control arm. Where randomised controls are not realistic, RWD-derived external controls can provide comparative context, and PMDA has accepted this approach in recent approvals. For example, lonafarnib was approved in January 2024 for Hutchinson-Gilford Progeria Syndrome, an ultra-rare condition where a randomised control group is not feasible, using international natural-history registry data as an external control.
Because the comparison does not come from a concurrent randomised group, this approach depends on careful design: comparable patient populations, a clear definition of index dates and follow-up windows, and transparent methods to manage confounding and bias. When these conditions are met, external controls can enable studies that would otherwise be infeasible.
Protocol optimisation using practice-based evidence
RWD also supports more practical and patient-aligned protocol design. Visit schedules, endpoint definitions, and follow-up requirements can often be refined to align more closely with how patients are monitored in Japan. That eases the burden on sites and supports more consistent data capture, and cleaner capture shows up directly in data quality.
Enhancing site selection through predictive analytics
Operational decisions can also benefit from RWD integration. When combined with historical performance and operational metrics, RWD can support site selection by identifying hospitals with sufficient eligible patient volume and relevant treatment experience. This can improve activation efficiency and reduce recruitment risk, and a more targeted site strategy often translates into faster study start-up and enrolment.
Supporting hybrid or decentralised trial models
Finally, RWD contributes to evolving trial delivery models. It helps teams understand how patients interact with the healthcare system outside scheduled trial visits, and that insight can support hybrid or decentralised elements, provided data governance and integrity requirements are clearly addressed.
Challenges to consider when applying RWD in Japan
RWD can improve trial planning, but it comes with practical constraints that teams should plan for early. Understanding these challenges early allows teams to plan appropriately and avoid delays or misinterpretation.
Data access limitations, privacy, and fragmentation
Access to high-quality datasets can involve complex approvals and strict privacy requirements. Fragmentation is also common: claims data may capture utilisation well but lack clinical outcomes, while EMRs offer detail but can be difficult to standardise across institutions.
Variability in EMR systems and coding practices
Differences in EMR platforms, coding conventions, and documentation practices introduce variability that must be addressed analytically. Local expertise is often essential to avoid misinterpretation, especially when translating clinical definitions into computable endpoints.
Practical recommendations for global trial teams
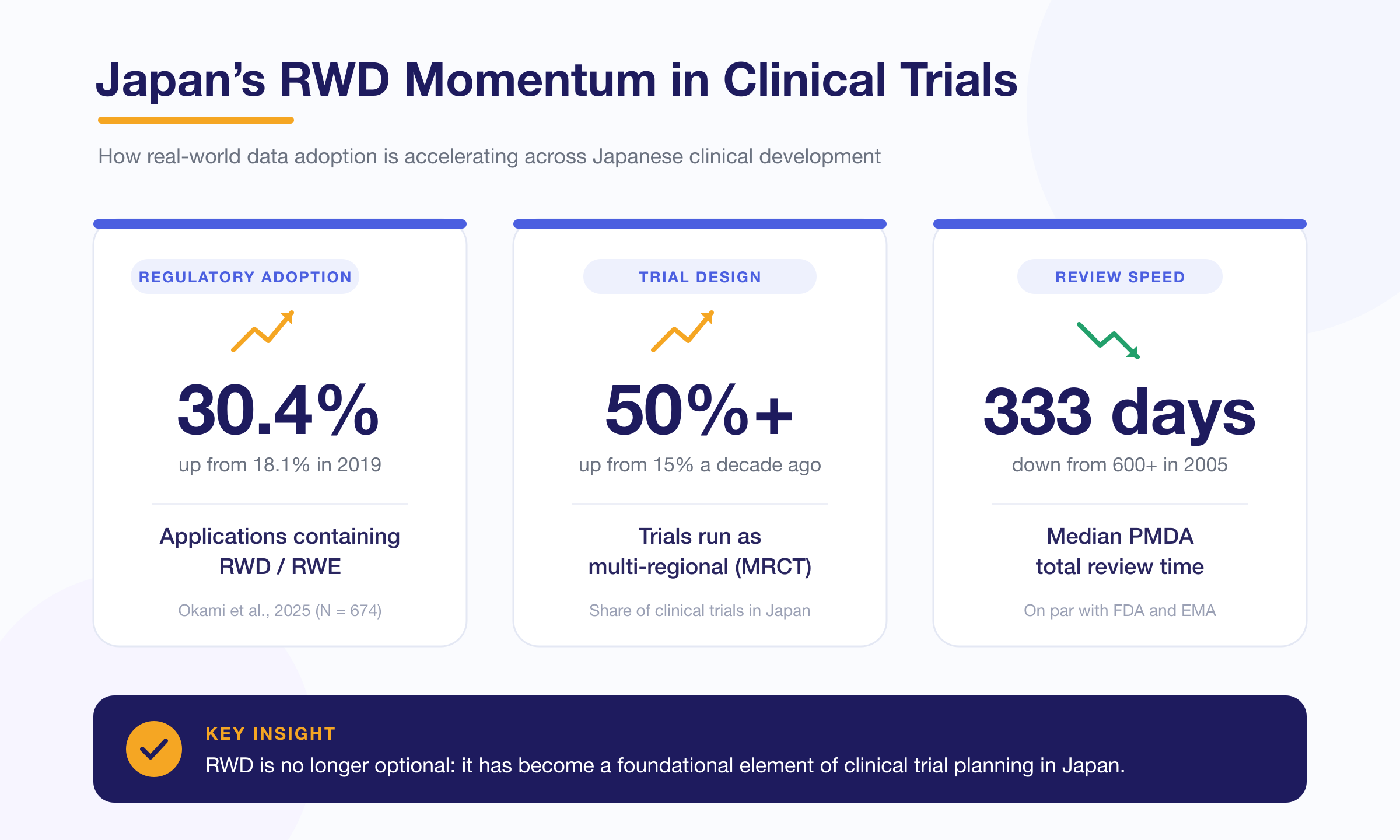
To use RWD effectively in Japan-focused clinical development, global teams should consider the following (noting that over 50% of clinical trials in Japan are now multi-regional clinical trials, compared with 15% ten years ago):
- Use PMDA consultations to confirm the role of RWD (feasibility only vs supportive evidence)
- Choose data sources based on the decision you need to make, such as prevalence estimates, endpoint feasibility, or site selection
- Work with local partners who understand Japanese care pathways and coding practices, especially when mapping endpoints
- Document methods clearly, including cohort selection logic, missingness handling, and confounding controls
Why RWD will continue reshaping clinical trials in Japan
Looking ahead, the role of RWD in Japan is likely to expand further. Its ecosystem is growing, and regulators are gaining more experience evaluating real-world evidence in context. Between 2019 and 2024, the proportion of regulatory applications containing RWD/RWE increased from 18.1% to 30.4%, signalling a clear trajectory. For sponsors planning trials in Japan, the value of RWD is straightforward: earlier clarity on feasibility, fewer protocol assumptions carried over from other regions, and trial designs that are better aligned with Japanese clinical practice.
Teams that build RWD into planning early are typically better positioned to reduce operational risk, engage regulators more effectively, and deliver studies that are both credible and executable in the Japanese setting. For sponsors serious about the Japanese market, early use of RWD is fast becoming standard practice in trial design rather than a differentiator.
For More Information, Please Contact Us Here
About Japanese Healthcare System

What you need to know about the healthcare system in Japan before using the data.
SERVICE

In addition to various web tools that allow you to easily conduct surveys via a browser using our medical database, we offer data provision services categorized into four types to meet your needs and challenges: "Analysis reports" "Datasets," "All Therapeutic Areas Data Provision Service," and "Specific Therapeutic Areas Data Provision Service.
![]()
© Medical Data Vision Co., Ltd. All Rights Reserved.